A three-part biomarker strategy aims to reduce one of neurology’s hardest diagnostic problems
Doctors have long struggled to distinguish among the major neurodegenerative disorders that cause parkinsonism. Parkinson’s disease, multiple system atrophy and progressive supranuclear palsy can look similar early on, yet they arise from different underlying protein pathologies and can progress in different ways. A new study published in Nature Medicine reports that a combined biomarker approach may move that diagnostic process closer to a biologically grounded test strategy rather than relying mainly on symptoms and clinical judgment.
The research evaluated three minimally invasive markers together: dermal alpha-synuclein seed amplification assays, dermal 4-repeat tau seed amplification assays, and serum neurofilament light chain. Instead of treating any one measure as a silver bullet, the investigators tested whether combining them could sort patients more accurately across disorders with overlapping clinical features and frequent co-pathology.
What the researchers studied
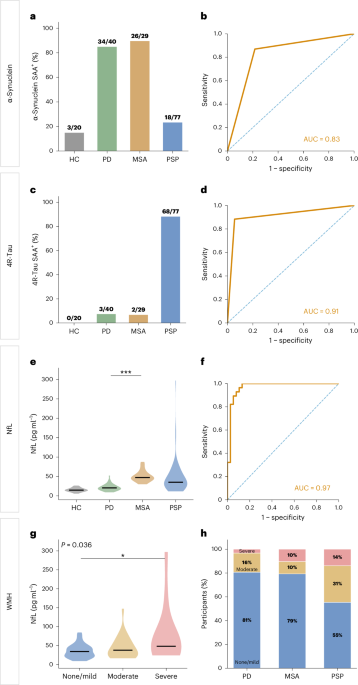
The prospective cohort included 166 participants: 40 with Parkinson’s disease, 29 with multiple system atrophy, 77 with progressive supranuclear palsy and 20 healthy controls. The team also used an independent external validation cohort of 63 participants. That design matters because biomarker studies often show promise in discovery groups but weaken when tested elsewhere. Here, the paper reports both initial performance and external validation.
The central problem is that parkinsonian syndromes are not cleanly separated by symptoms alone. Tremor, rigidity, slowed movement, balance problems and cognitive changes can overlap. On top of that, some patients carry more than one protein pathology, making interpretation of single-protein biomarkers more difficult. The study therefore focused on complementary signals rather than a winner-take-all test.

How the markers performed
The alpha-synuclein assay identified synucleinopathies with high sensitivity, consistent with its intended role in flagging disorders such as Parkinson’s disease and multiple system atrophy. But the paper also reports alpha-synuclein positivity in a subset of progressive supranuclear palsy cases, which the authors say is consistent with co-pathology rather than a simple classification error. That finding reinforces a broader point in neurodegeneration: biology does not always follow the tidy boundaries used in clinical labels.
The 4-repeat tau assay, run on dermal samples, identified progressive supranuclear palsy with high sensitivity and specificity. That gives clinicians a potentially useful counterweight to alpha-synuclein testing, particularly when patients present with ambiguous movement symptoms that could reflect either a synucleinopathy or a tauopathy.
Serum neurofilament light chain added another layer. In the study, it helped distinguish multiple system atrophy from Parkinson’s disease and also correlated with disease severity in progressive supranuclear palsy. Neurofilament light is not disease-specific, but it can reflect neuroaxonal injury burden. In this setting, it appears to have improved separation where protein-seeding assays alone could not fully resolve the picture.
Why the combined approach matters
The main finding is not simply that each marker works in isolation. It is that integrating them improved diagnostic discrimination compared with individual markers alone. The paper also says the approach enabled additional stratification within progressive supranuclear palsy, suggesting it may help identify biologically meaningful subgroups inside a diagnosis that often appears clinically heterogeneous.
That matters for several reasons. More accurate early diagnosis can improve counseling, care planning and trial enrollment. Drug development in neurodegeneration increasingly depends on matching therapies to the right underlying pathology. If a patient’s syndrome is misclassified at entry, both the trial and the interpretation of results can suffer. A multimodal biomarker panel could therefore become useful not only in clinics but in study design for future disease-modifying therapies.
The fact that the assays are described as minimally invasive is also important. Skin-based biomarkers and blood markers are more scalable than procedures that require more burdensome sampling or advanced imaging infrastructure. If future validation holds up, such tools could be easier to deploy in specialized movement-disorder centers and possibly beyond them.

Caution remains
The study does not eliminate uncertainty. The source text emphasizes the challenge of overlapping pathology, and even the positive alpha-synuclein findings in some progressive supranuclear palsy patients show that biomarkers can reveal mixed biology rather than a neat answer. That may ultimately be a strength, but it also complicates how clinicians communicate results and how diagnostic thresholds are set.
The cohort sizes, while substantial for this type of work, are still moderate relative to the diversity seen in real-world neurology practice. Broader deployment would require further confirmation across additional sites, patient populations and disease stages. It will also matter to learn how these tests perform in very early disease, when symptoms are subtle and the clinical need for clarity is often greatest.
Still, the study points in a clear direction. Instead of searching for one definitive biomarker to sort all parkinsonian disorders, the field may be moving toward layered panels that reflect the messy biological reality of neurodegeneration. In that framework, diagnostic precision comes from combining orthogonal signals: one marker for synuclein, another for tau, and a third for injury burden.
A step toward biologically informed diagnosis
The authors conclude that their findings support a multimodal biomarker approach for biologically informed diagnosis of parkinsonian syndromes. That phrasing is deliberate. The study is not promising a one-test solution or instant certainty. It is arguing for a more grounded way to classify disease, one that aligns symptoms with measurable pathology.
For clinicians, that could mean fewer diagnostic dead ends. For patients, it could mean faster and more confident answers. And for the wider neurodegeneration field, it offers a practical example of how skin and blood biomarkers might be combined to make difficult diagnoses less dependent on inference alone.
This article is based on reporting by Nature Medicine. Read the original article.

Originally published on nature.com