An outbreak escalates within days
The World Health Organization has declared the current Ebola outbreak a public health emergency of international concern after cases and deaths mounted rapidly in the Democratic Republic of the Congo and crossed into neighboring Uganda. The declaration reflects both the outbreak’s immediate scale and the unusual risks attached to the virus strain involved.
According to data cited from the US Centers for Disease Control and Prevention for May 17, the DRC had recorded 10 confirmed cases, 336 suspected cases and 88 deaths. Uganda had reported two confirmed cases and one death. Even at this early stage, those figures place the outbreak among the 10 largest Ebola outbreaks on record by size, though still far below the 2014 to 2016 West African crisis.
The WHO stressed that the situation does not meet the criteria for a pandemic emergency. But a public health emergency of international concern is still the organization’s highest formal alarm for cross-border disease events. It signals that the outbreak demands a coordinated international response because it poses risks beyond one country’s borders.
Why health authorities are alarmed
In explaining the declaration, WHO Director-General Tedros Adhanom Ghebreyesus cited more than raw case counts. The outbreak has produced clusters of suspected cases and deaths across multiple DRC health zones, including deaths among healthcare workers. Officials also say some geographically distant cases do not appear to have clear epidemiological links, suggesting transmission may be broader than current surveillance has captured.
That uncertainty matters. Ebola response efforts depend heavily on tracing chains of infection, isolating cases and containing spread quickly. When cases emerge without obvious connections, it raises the possibility that the visible outbreak is only a fraction of the true one. The WHO also pointed to insecurity, humanitarian pressures, population mobility, urban or semi-urban hotspots and widespread informal healthcare networks as factors that could accelerate regional transmission.
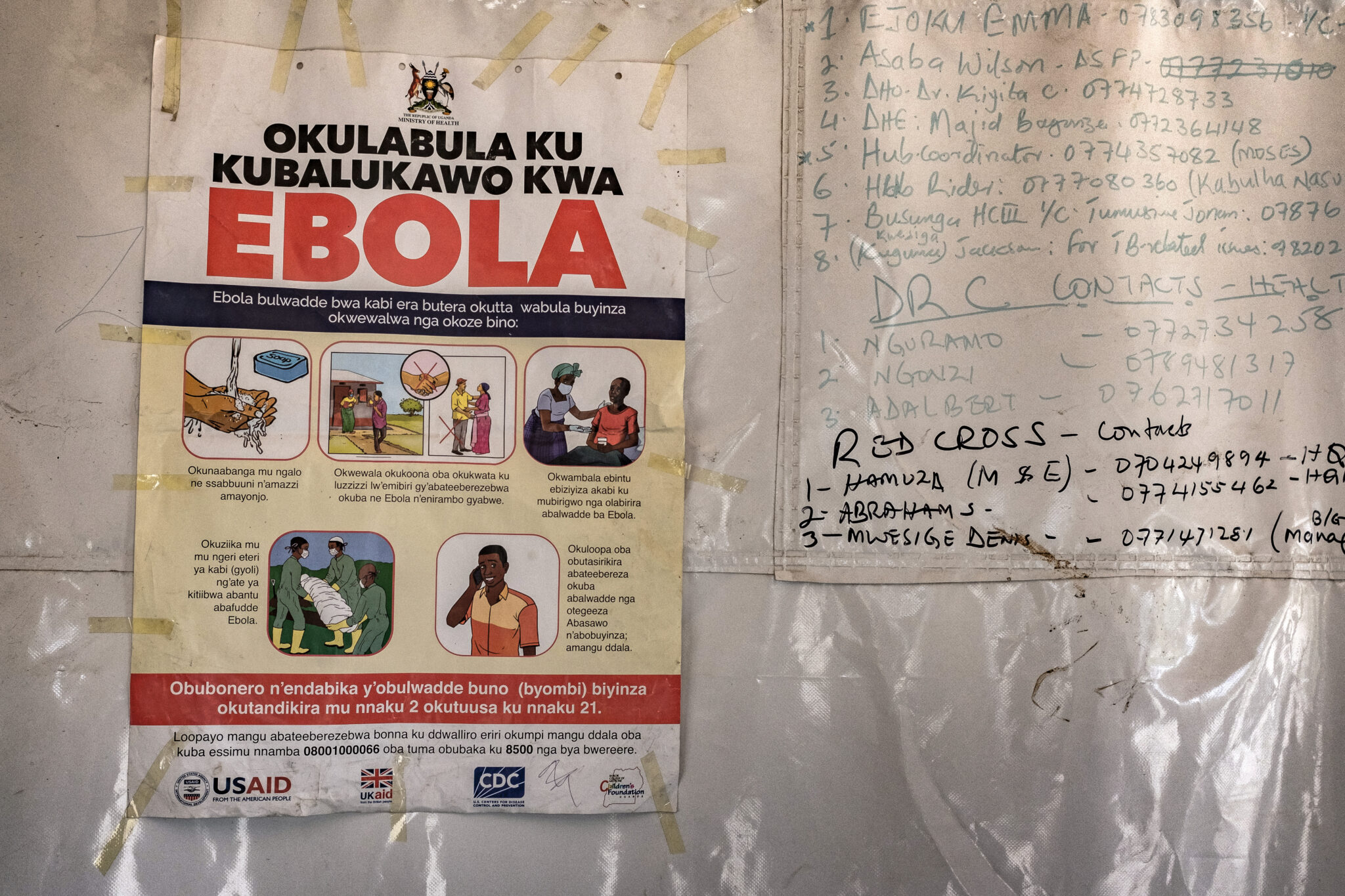
These are conditions that can frustrate even experienced response systems. Mobility can move infections across borders before contacts are identified. Conflict and instability can block response teams from reaching affected areas. Informal healthcare settings can become transmission points if infection-control procedures are limited. Taken together, those factors explain why an outbreak that initially appeared localized has already been treated as a multinational emergency.

The Bundibugyo strain raises the stakes
Another reason for concern is the virus itself. This outbreak is caused by the Bundibugyo strain of Ebola virus, an uncommon form that has caused only two previous outbreaks. The strain has historically shown fatality rates of roughly 25 percent to 50 percent, according to the supplied source text.
What makes Bundibugyo especially challenging is that it lacks clinically validated treatments or vaccines. For the more common Zaire strain, the world now has established vaccines and therapeutics, a major change from the early years of Ebola response. Bundibugyo does not offer that advantage. That means public health authorities are leaning more heavily on classical outbreak control tools such as surveillance, isolation, border monitoring and supportive care, rather than being able to deploy proven strain-specific medical countermeasures.
The combination of a less familiar strain and a fast-moving cross-border pattern helps explain why authorities moved so quickly. A virus that spreads in difficult operating conditions is dangerous enough. A virus without validated treatments or vaccines adds another layer of urgency.
International measures are already tightening
The international response has begun to harden around travel controls and patient movement. The source text says the United States has restricted travel and that the CDC is working to move an infected American and six others to Germany. Those actions indicate concern not just about local containment but also about protecting international transport systems and ensuring access to high-level care for exposed or infected individuals linked to US operations.
Travel restrictions alone do not stop outbreaks, and they can introduce their own complications. But in a rapidly evolving event involving cross-border spread, they often become part of a broader effort to reduce risk while surveillance and case management systems scale up.
The immediate test now is whether health authorities can close the gap between suspected and confirmed cases, reconstruct missing chains of transmission and protect frontline workers. Four healthcare worker deaths, as cited by WHO, are a stark warning sign. They suggest that clinical settings are already under strain and that infection prevention protocols may be under pressure in affected zones.

What to watch next
The key questions in the coming days are straightforward. Are suspected cases being confirmed at a pace that clarifies the outbreak’s true size? Can health teams identify the links between distant clusters? Does Uganda remain limited to the cases already reported, or will wider cross-border spread emerge? And can authorities contain transmission without the help of validated vaccines or treatments for this strain?
For now, the WHO declaration reflects a sober calculation: the outbreak is already large, likely underdetected and unfolding in conditions that make containment harder. It is not yet being treated as a pandemic event, but it has clearly moved beyond the threshold of a routine regional flare-up.
That distinction matters. A public health emergency of international concern is meant to trigger attention before the worst-case scenario arrives. In the case of this Ebola outbreak, global health officials are signaling that waiting longer would have been the riskier choice.
This article is based on reporting by Ars Technica. Read the original article.
Originally published on arstechnica.com