A first clinical test of a disease-specific approach
Preeclampsia remains one of the most dangerous complications of pregnancy, particularly when it emerges early enough to force delivery far before term. In a pilot trial published in Nature Medicine, researchers tested an experimental strategy designed to lower levels of soluble Fms-like tyrosine kinase 1, or sFlt-1, a placental protein widely implicated in the disease process. The study does not establish a new standard of care, but it offers an early sign that a targeted, mechanism-based intervention may be possible in a condition where treatment options have long been limited.
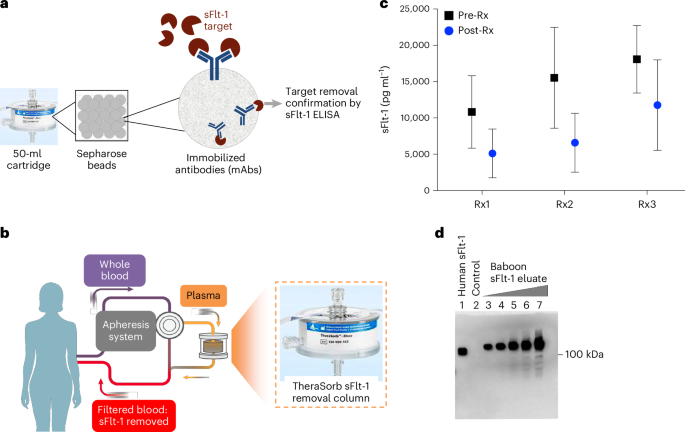
The investigators developed an antibody-based apheresis approach intended to selectively remove circulating sFlt-1 from the mother’s blood. Their report describes preclinical work in pregnant baboons and an open-label, single-arm human study in women with preterm and very preterm preeclampsia. The trial’s primary focus was not proof of efficacy, but safety and tolerability.
Why sFlt-1 matters
The rationale for the study is straightforward. The paper states that sFlt-1 plays a central role in the pathogenesis of preeclampsia. That makes it an unusually attractive therapeutic target: not just a marker associated with the condition, but a factor believed to help drive it. In preeclampsia, clinicians often have to balance maternal risk against fetal immaturity, because there is no disease-specific treatment that reliably halts the underlying process.
A therapy that could reduce the biological pressure of the disease, even temporarily, could matter most in pregnancies where every additional day in utero has clinical value. The authors therefore focused on women with very preterm disease, where prolonging pregnancy, stabilizing maternal status, or both could be meaningful.

What the pilot trial found
In the preclinical portion, extracorporeal apheresis using an adsorber containing high-affinity IgG1 antibodies against sFlt-1 produced about a 50% reduction in circulating sFlt-1 levels in pregnant baboons. That result established a proof of principle that the system could selectively lower the target protein.
The human study was divided into phases. In phase A, seven women with preterm preeclampsia received single ascending doses. According to the paper, maternal and fetal vital signs and umbilical artery pulsatility indices remained stable when comparing measures before, during, and after apheresis. That is an important early observation for a therapy used in a high-risk pregnancy setting, where any intervention must be judged not only by maternal laboratory effects but also by fetal tolerance.
In phase B, nine women with very preterm preeclampsia received multiple doses. The paper reports a median gestational age of 30.3 weeks in this group. Each apheresis session reduced sFlt-1 levels by an average of 16.7%, and mean arterial pressure fell by an average of 4.1 mmHg. The authors also report a correlation between reductions in blood pressure and reductions in circulating sFlt-1, suggesting that the biological target engagement may be connected to the observed hemodynamic effect.
How to read the results
The findings are promising, but they should be interpreted within the limits of a pilot study. The trial was open-label and single-arm, with small patient numbers. It was designed to look first at whether the procedure could be performed safely and whether it produced the expected biological effect. It was not built to determine whether the intervention improves hard clinical outcomes such as maternal complications, neonatal survival, or meaningful prolongation of pregnancy.
That distinction matters. In obstetric medicine, even biologically elegant interventions can fail to translate into outcomes that change practice. The modest average blood-pressure reduction reported here is interesting, but it is not, by itself, enough to show that the therapy alters the course of disease in a way that justifies wider use.
Still, the study’s importance lies in what it makes testable next. It advances a long-standing scientific idea, that preeclampsia may be addressed by directly modifying a circulating pathogenic factor, into human clinical evidence. For a field that often relies on surveillance and timed delivery rather than disease-specific treatment, that is a notable step.

What could come next
The most immediate next question is whether selective sFlt-1 removal can produce durable clinical benefit in a larger, controlled trial. Future studies would need to measure endpoints that matter to patients and clinicians alike: whether pregnancies can be safely prolonged, whether severe maternal complications are reduced, and whether neonatal outcomes improve.
Researchers will also need to determine which patients, if any, are most likely to benefit. Preeclampsia is a syndrome with varying severity, timing, and biological features. If sFlt-1 is especially relevant in a particular subgroup, that may shape how later trials are designed. The practical burden of repeated apheresis, including infrastructure, monitoring, and cost, will also influence whether the approach can move beyond specialized centers.
There is also a broader scientific implication. Pregnancy complications have historically received less drug-development attention than many other serious conditions, partly because of safety complexity and the challenge of conducting interventional studies during pregnancy. A targeted therapy that can be mechanistically justified and carefully monitored may help shift that landscape.
An early but meaningful signal
This pilot trial does not solve preeclampsia. What it does provide is an early clinical signal that a disease-linked protein can be selectively depleted in pregnant patients without obvious immediate instability in the study setting, while producing measurable reductions in both sFlt-1 and blood pressure. That is enough to justify deeper investigation.
For now, the work stands as a careful first move toward a more specific treatment model for a life-threatening pregnancy disorder. If larger trials confirm benefit, the field may eventually gain something it has lacked for decades: a therapy aimed not just at managing the consequences of preeclampsia, but at intervening in its biology.
This article is based on reporting by Nature Medicine. Read the original article.

Originally published on nature.com