A Preventable Crisis
A sweeping analysis of global cancer incidence data from 185 countries has concluded that approximately four in ten cancer cases worldwide are attributable to modifiable risk factors—behaviors, exposures, and conditions that people and healthcare systems can potentially change. The study, published in Nature Medicine, represents one of the most comprehensive assessments of preventable cancer burden ever conducted and identifies specific risk factors and geographic regions where targeted interventions could have the greatest impact.
The findings carry significant implications for cancer prevention policy. Unlike genetic risk factors, which individuals cannot change, modifiable risk factors are targets for public health campaigns, regulatory action, clinical screening, and lifestyle interventions. If even a fraction of the 40 percent attribution can be translated into actual prevented cases, the global cancer burden could be substantially reduced.
The Major Risk Factors
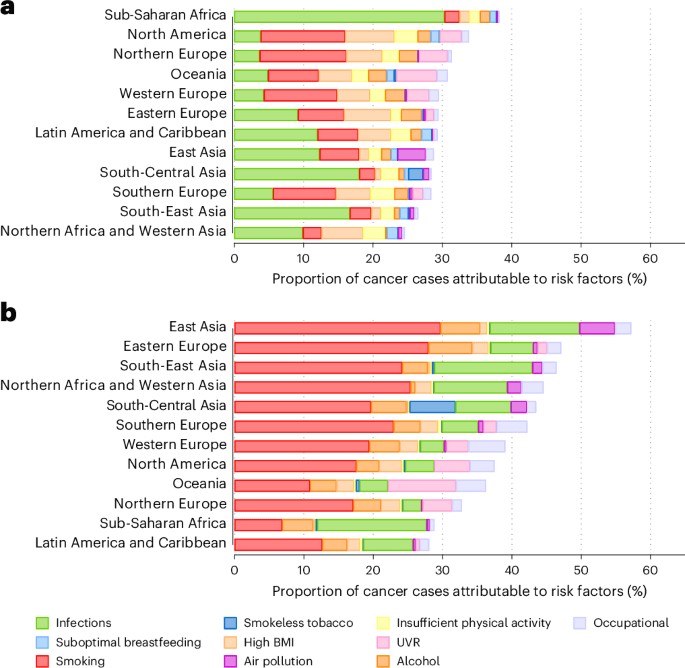
The study examined a range of risk factors using standardized epidemiological methods, attributing fractions of each cancer type to each factor based on the evidence for causal relationships and the prevalence of the risk factor in each country. The leading contributors to modifiable cancer burden include tobacco use—still the single largest preventable cause of cancer globally—excess body weight, alcohol consumption, physical inactivity, and infection with cancer-causing pathogens including human papillomavirus (HPV), hepatitis B and C viruses, and Helicobacter pylori bacteria.
Environmental exposures—air pollution, ultraviolet radiation, and certain occupational carcinogens—also contribute meaningfully to the burden, though they are less amenable to individual behavior change and more dependent on regulatory and infrastructure interventions.
Geographic and Sex-Specific Variation
One of the study's most important contributions is documenting how the pattern of risk-attributable cancer varies substantially by region and sex. In high-income countries, obesity and alcohol-related cancers are disproportionately represented. In low- and middle-income countries, infection-driven cancers—cervical cancer caused by HPV, liver cancer caused by hepatitis B and C, and stomach cancer caused by H. pylori—contribute a much larger share of the preventable burden.
This geographic variation means that prevention strategies effective in one setting may not translate directly to another. A wealthy country's focus on obesity prevention and smoking cessation programs would need to be adapted for a lower-income setting where vaccination against HPV and hepatitis B, and antibiotic treatment of H. pylori, offer larger potential gains.
Implications for Prevention Investment
The 40 percent attribution figure, while striking, understates the prevention opportunity because it reflects only the current level of risk factor prevalence. If tobacco use, obesity rates, and other risk factors continue on their historical trajectories, the preventable fraction could grow. Conversely, successful prevention programs could reduce the fraction over time.
The study argues explicitly for "targeted, population-level interventions adapted to regional and sex-specific risk profiles" rather than one-size-fits-all global campaigns. In practice, this means national health authorities should use their country-specific risk factor data to prioritize interventions where the evidence base for benefit is strongest relative to local burden.
The Screening and Early Detection Layer
Beyond primary prevention—reducing exposure to risk factors—secondary prevention through screening and early detection plays an important complementary role. Cancers detected at early stages have substantially better survival rates than those caught after metastasis. Cervical cancer, colorectal cancer, breast cancer, and lung cancer in high-risk individuals all have established screening programs with demonstrated mortality benefits.
Expanding access to screening in low-income settings, where rates of advanced-stage diagnosis remain high, could reduce cancer mortality even independently of risk factor reduction. The combination of primary prevention targeting modifiable risk factors and secondary prevention through screening offers a two-pronged strategy for reducing cancer's global toll.
The Infection-Cancer Link
Infection-attributable cancers deserve particular attention because they are preventable through vaccination and treatment at relatively low cost. HPV vaccination programs have already demonstrated dramatic reductions in cervical pre-cancers in countries with high coverage. Hepatitis B vaccination, widely deployed in childhood immunization programs, has reduced rates of hepatitis B-related liver cancer in vaccinated birth cohorts. H. pylori eradication therapy reduces stomach cancer risk in infected individuals.
Scaling these interventions globally—particularly the HPV vaccine, whose coverage remains low in many high-burden countries—could prevent millions of cancer cases annually. The study's data provide a rigorous foundation for the economic case that investing in these interventions would yield substantial returns in reduced cancer burden and associated healthcare costs.
This article is based on reporting by Nature Medicine. Read the original article.


