Bespoke gene therapies are moving from theory to practice
Rare pediatric diseases are no longer being treated only as scientific curiosities. In a new correspondence published in Nature Medicine, a group of researchers argues that they are increasingly becoming candidates for custom-built cell and gene therapies, including treatments designed for a single patient.
The authors point to a striking recent shift. Inherited disorders that were once effectively untreatable are now seeing one-time gene therapies produce meaningful and durable benefits. That change is significant on its own, but the paper argues that the larger disruption is structural: regulators, developers, and health systems are now confronting medicines that do not fit the assumptions of conventional drug development.
According to the correspondence, single-patient trials are no longer hypothetical. The authors cite one ultra-rare neurological disease in which a tailored adeno-associated virus gene therapy was developed and administered within three years. They also highlight an even faster case in which a patient-specific base-editing therapy was created, cleared by regulators, and delivered to a newborn with a lethal metabolic disorder in roughly eight months.
Those examples suggest that the scientific and manufacturing side of individualized therapy is advancing quickly. The harder problem, the authors argue, is building a pathway that can make these treatments reachable for more children rather than just a handful of extraordinary cases.
The access problem is now economic as much as scientific
The correspondence frames access as the central bottleneck. Even as custom gene therapies become more feasible, most children with rare diseases still do not have access to effective treatment. The paper does not describe that gap as a failure of science alone. Instead, it argues that the conventional commercial model for pharmaceuticals is poorly matched to highly individualized therapies.
That mismatch is already visible in the market. The authors note that biotech companies that helped pioneer gene therapies have struggled to remain commercially viable, and in some cases have withdrawn products despite lifesaving efficacy. In other words, the problem is not simply whether a therapy can work. It is whether the institutions built to finance, approve, manufacture, and sustain treatments can support products aimed at extremely small patient populations, or even a single child.
That creates a contradiction at the heart of the field. The more precisely a therapy is tailored, the less it resembles the kind of scalable product that the traditional for-profit drug model is designed to reward. For common diseases, large trials and broad markets can justify years of investment. For ultra-rare pediatric disorders, that same model can become a barrier rather than an engine.
The correspondence argues that unless the system changes, individualized therapies may continue to appear as isolated breakthroughs rather than a dependable treatment category.

A framework meant to bridge development and regulation
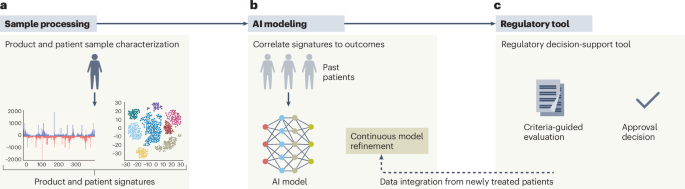
The paper introduces what it calls the UNICORN framework, presented as a route from product characterization to regulatory decision-making. The correspondence excerpt provided here does not spell out every operational detail of that framework, but its purpose is clear from the authors’ argument: create a repeatable structure for evaluating bespoke gene therapies without forcing them into approval pathways built for mass-market drugs.
That matters because the standard model depends heavily on large cohorts, repeatable manufacturing runs, and extensive commercial validation. Ultra-rare pediatric therapies may have none of those features. A regulator still has to weigh quality, safety, and likely benefit, but the evidence package may need to look different when the treatment is designed around one child’s mutation, timeline, and clinical trajectory.
The correspondence therefore points toward a more adaptive model, one that can connect product characterization and regulatory review in a way that preserves rigor while acknowledging that individualized therapies are fundamentally different products.
The underlying message is not that standards should be weakened. It is that standards may need to be translated into a new format. If a therapy is made for one patient, then the approval logic cannot rely on the same assumptions used for a product intended for tens of thousands.
Why pediatric rare disease is the pressure point
Pediatric rare disease is where this pressure is most acute. The patients are few, the progression can be fast, and delays can carry lifelong consequences. The two examples cited by the authors underscore that urgency. A three-year development timeline for a tailored therapy is already unusually compressed by historical drug-development standards. An eight-month path from design to regulatory clearance to treatment in a newborn is more dramatic still.
Those timelines show both the promise and the fragility of the field. They demonstrate that bespoke therapies can move with remarkable speed when science, manufacturing, regulation, and clinical need align. They also raise a difficult question: if this can happen in exceptional cases, what would it take to make it happen systematically?
The correspondence argues that the answer is not simply more laboratory innovation. It is also better institutional design. Pediatric rare diseases often have no fallback treatment and no large commercial market. That makes them a test case for whether medicine can build development systems around need rather than scale.

What this proposal signals for the field
The significance of the paper lies less in announcing a single therapy than in acknowledging that a new category of medicine is arriving faster than legacy systems can absorb it. The authors describe a world in which bespoke gene therapies are becoming technically possible, clinically meaningful, and yet structurally difficult to deliver.
If their argument holds, future progress in rare pediatric disease will depend not only on better vectors, editing tools, or manufacturing methods, but also on approval pathways that recognize individualized therapies as a durable reality. The correspondence makes the case that rare-disease medicine has entered that phase already.
That is an important shift. For years, personalized gene therapy often sounded like a frontier ambition. The examples cited here suggest it is now becoming an administrative and regulatory challenge as much as a scientific one. The next breakthroughs may depend on whether regulators and developers can turn one-off successes into a workable system.
For families confronting devastating childhood disorders, that distinction is not abstract. It could determine whether bespoke medicine remains the exception, or starts to become part of routine care for diseases too rare to fit the old model.
This article is based on reporting by Nature Medicine. Read the original article.
Originally published on nature.com